Quick Answer: PET Scan vs CT Scan in One Paragraph
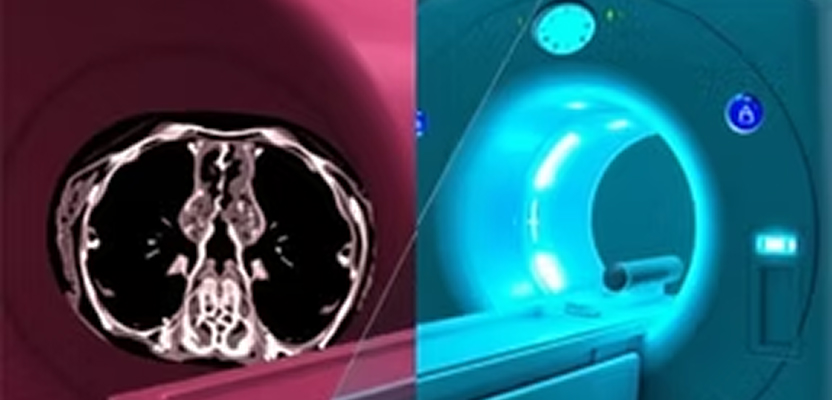
A CT (computed tomography) scan uses X-rays to produce detailed anatomical images — it shows what organs, bones, and tissues look like. A PET (positron emission tomography) scan uses a small dose of an injected radioactive tracer to show how cells and tissues function — particularly how much sugar they consume, which makes cancers, infections, and underperfused heart muscle stand out. Most modern scanners combine both technologies into a single PET/CT scan, which overlays metabolic activity on top of anatomy in one study. The choice between them depends on the clinical question: structural problem (CT) vs. functional or metabolic problem (PET).
The five differences in 30 seconds:
- What they show: CT shows anatomy and structure. PET shows metabolism and cell-level activity.
- How they work: CT uses X-rays. PET uses an IV-injected radiotracer (most commonly FDG, a glucose analog).
- Most common uses: CT for trauma, stroke, lung nodules, and acute pain. PET for cancer staging, viable heart tissue, and certain neurological conditions.
- Time: CT takes 5 to 30 minutes total. PET/CT takes 2 to 3 hours total (most of it is the tracer uptake wait),
- Radiation: A typical CT delivers 2 to 10 mSv. A combined PET/CT delivers around 25 mSv, depending on protocol.

Bring Mobile Cardiac PET to Your Practice
If you are a physician evaluating whether to order a CT, a PET, or both — or a patient who has just been told you need one — keep reading. Below we walk through every difference that matters, the cardiac PET use case that is reshaping nuclear cardiology in 2026, and the specific questions patients ask most often.
What Is a CT Scan?
A computed tomography scan, often called a CT or CAT scan, is an imaging test that uses a rotating X-ray beam and a computer to assemble cross-sectional ("slice") images of the body. Each slice is roughly the thickness of a coin, and modern multi-detector CT scanners can capture an entire chest or abdomen in under a minute.
CT excels at showing structural detail. It is the imaging workhorse of emergency rooms because it can quickly identify bleeding in the brain, fractures, blood clots in the lungs (pulmonary embolism), kidney stones, ruptured organs, and tumors that have changed the size or shape of an organ. Contrast dye — usually an iodine-based agent given through an IV — can be added to highlight blood vessels, the lining of the bowel, or organs like the kidneys and liver.
A typical CT scan takes 5 to 30 minutes from the time you walk into the room. The actual image acquisition is usually under a minute. Patients lie on a table that slides through a doughnut-shaped gantry; nothing touches you.

What Is a PET Scan?
A positron emission tomography scan is a nuclear medicine test that maps biological activity rather than structure. Before the scan, a small amount of a radioactive tracer is injected into a vein. The tracer is built around a biologically interesting molecule — most commonly fluorodeoxyglucose (FDG), a glucose analog. Cells that consume glucose rapidly (such as most cancers, infections, and active brain or heart tissue) take up more tracer. The PET scanner detects the tiny gamma-ray emissions from the tracer and reconstructs a map of where it accumulated.
Because PET measures function, it can identify disease before it has changed the shape of an organ. A 5-millimeter tumor that is metabolically active can light up on PET while still being undetectable on CT. Conversely, scar tissue with no blood flow looks "cold" on PET — which is exactly the information a cardiologist needs when deciding whether a patient's heart muscle is salvageable.
The full PET appointment is longer than CT — typically two to three hours. Most of that is the uptake phase: after the IV injection, you rest quietly for 45 to 60 minutes while the tracer circulates and accumulates. The actual scan itself takes about 20 to 40 minutes, according to the American College of Radiology and StatPearls (NCBI).
PET Scan vs. CT Scan: The 7 Key Differences
At the level of clinical decision-making, here is what separates the two tests:
- What it images: CT shows anatomy and structure; PET shows metabolism and cellular function.
- Radiation source: CT uses an external X-ray beam; PET uses an injected radioactive tracer (such as FDG or Rb-82).
- Best for: CT excels at trauma, fractures, bleeding, structural tumors, and lung nodules. PET excels at cancer staging, viable myocardium, and dementia work-up.
- Typical time: CT takes 5 to 30 minutes total. PET takes 2 to 3 hours total (45-minute uptake plus 20 to 40 minutes of scanning).
- Effective radiation dose: 2 to 10 mSv for CT; 5 to 8 mSv for PET alone; approximately 25 mSv for combined PET/CT.
- Contrast: CT often uses iodinated IV contrast. PET does not require separate contrast — the tracer is the agent.
- Disease detection before structural change: CT requires a visible structural change to detect disease. PET picks up metabolic change first, sometimes months earlier.
The strength of a CT is precision about what something looks like. The strength of a PET is precision about what something is doing. That is why so many oncology, cardiology, and neurology workflows order them together as PET/CT — anatomy and function fused into a single image.
When Do Doctors Order a CT Scan?
CT is the right answer when the clinical question is structural. The most common indications include:
- Trauma and emergency care: head injury, suspected internal bleeding, fractures.
- Acute abdominal pain: appendicitis, kidney stones, bowel obstruction, diverticulitis.
- Lung evaluation: pulmonary embolism, lung nodules, lung cancer screening with low-dose CT.
- Cardiac structural and coronary imaging: coronary CT angiography (CCTA) to look at the coronary arteries directly, plus calcium scoring.
- Stroke work-up: non-contrast CT of the head is the first-line test in suspected acute stroke.
- Initial cancer detection: identifying masses and characterizing organ size.
CT is fast, widely available, and inexpensive relative to PET. For many emergencies it is the only imaging test a patient will need.
When Do Doctors Order a PET Scan?
PET is the right answer when the clinical question is functional or metabolic. The most common indications include:
- Cancer staging and re-staging: determining whether a known cancer has spread to lymph nodes or distant sites.
- Treatment response: evaluating whether chemotherapy or radiation is working before the tumor changes size.
- Cancer recurrence: distinguishing scar tissue from active disease in a treated patient.
- Cardiac perfusion and viability: myocardial perfusion imaging with Rb-82 or N-13 ammonia, plus viability imaging with FDG.
- Neurology: differentiating Alzheimer's from other dementias, locating seizure foci before epilepsy surgery, and evaluating Parkinsonian syndromes.
- Fever or infection of unknown origin: localizing inflammation when other tests have failed.
According to a meta-analysis published in Circulation: Cardiovascular Imaging, cardiac PET myocardial perfusion imaging shows pooled sensitivity and specificity of approximately 89 to 92 percent and 86 to 90 percent — meaningfully higher than SPECT (83 to 88 percent sensitivity, 74 to 85 percent specificity) for the diagnosis of coronary artery disease.
The Combined PET/CT Scan: When You Need Both
Most modern PET scanners are physically combined with a CT scanner in the same gantry. During a PET/CT exam, the CT portion is acquired first (usually a low-dose, non-diagnostic CT used for attenuation correction and anatomical reference), and the PET portion is acquired immediately afterward without the patient leaving the table. The two image sets are then fused, so a hot spot of metabolic activity is overlaid on the exact anatomical location it came from.
The clinical advantage is precision. A PET image alone might show that something in the chest is metabolically hot, but a fused PET/CT shows that the hot spot is a 9-mm lymph node in the right hilum — information you can act on. PET/CT has become the standard of care for staging most solid tumors and for certain cardiac and neurology workflows.
For Medicare and most commercial payers, PET/CT is reimbursed as a single bundled study with specific CPT codes for the body region and clinical indication. (See our 2026 Cardiac PET/CT Reimbursement Guide for code-by-code reimbursement detail in the cardiology setting.)
Cardiac PET vs. Cardiac CT: A Specialized Comparison
This is the comparison that matters most for cardiologists in 2026 — and it is the one that most general PET vs. CT articles miss entirely.
Cardiac CT (CCTA) uses X-ray and IV iodinated contrast to visualize the coronary arteries directly. It excels at anatomy: identifying coronary plaque, characterizing stenosis, and ruling out obstructive coronary artery disease in low- to intermediate-risk patients. It is structural.
Cardiac PET uses a perfusion tracer (most commonly Rubidium-82 or N-13 ammonia) to measure how much blood actually reaches the heart muscle at rest and under pharmacologic stress. It can also quantify myocardial blood flow (MBF) in absolute units (mL/min/g) and calculate coronary flow reserve (CFR) — measurements that no other modality can produce non-invasively. It is functional.
In practice:
- Use cardiac CT to ask, Are the coronary arteries narrowed?
- Use cardiac PET to ask, Is the heart muscle actually getting enough blood?
For many patients — particularly those with intermediate pretest risk, prior equivocal SPECT, body habitus that limits SPECT image quality, or known multivessel disease — cardiac PET is the more accurate test. A growing body of evidence and the latest SNMMI/ASNC/SCCT joint guidelines position PET myocardial perfusion imaging as the most accurate non-invasive test for coronary artery disease in selected populations.
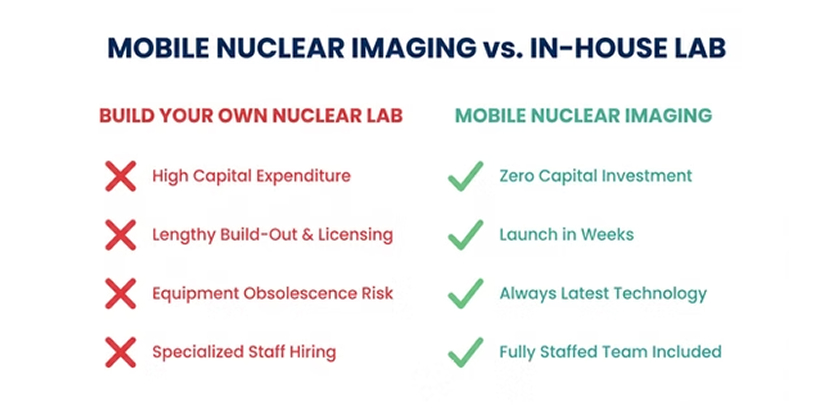
The historical barrier was access — fixed PET scanners were rare outside major academic centers, and patients had to be referred out. Mobile cardiac PET has changed that equation: a fully credentialed PET/CT scanner can come directly to a cardiology practice on scheduled days, allowing the practice to keep referrals in-house, retain patients across the imaging episode, and capture the full reimbursement of the study.

How Much Does a PET Scan vs. CT Scan Cost?
Costs vary enormously by setting (hospital outpatient vs. independent imaging center), payer, and region. Public US data published by GoodRx and the American Journal of Roentgenology puts the typical ranges at:
- CT scan (one body region, with contrast): roughly $300 to $1,500 at an outpatient imaging center; $1,000 to $3,500 at hospital outpatient; self-pay typically $300 to $3,500.
- PET/CT scan: roughly $1,200 to $6,000 at an imaging center; $4,000 to $18,000 at a hospital; self-pay typically $1,300 to $12,000 or more.
Medicare reimbursement is more consistent. A typical outpatient PET/CT in 2026 reimburses several thousand dollars at the 80 percent Medicare allowable, depending on the CPT bundle and locality. Cardiac PET/CT specifically reimburses approximately 4.2 times the rate of a comparable SPECT study through the same payer — a financial gap that drives much of the current shift from SPECT to PET in nuclear cardiology. (Detailed numbers, code-by-code, are in our Cardiac PET Reimbursement 2026 Guide.)
Radiation, Safety, and Side Effects
Both CT and PET use ionizing radiation, and both are considered safe when ordered for an appropriate clinical reason. The benefit of an accurate diagnosis nearly always outweighs the small statistical risk associated with the dose of a single scan.
For context, the average American is exposed to about 3 mSv per year of natural background radiation, according to the American Cancer Society. Typical effective doses are:
- Chest X-ray: about 0.1 mSv.
- Head CT: about 2 mSv.
- Chest CT: about 7 mSv.
- Abdomen and pelvis CT: 8 to 10 mSv.
- FDG PET alone: 5 to 8 mSv.
- Combined whole-body FDG PET/CT: about 25 mSv.
- Cardiac PET (Rb-82 rest/stress): 3 to 5 mSv — often lower than SPECT.
Note that cardiac PET with Rb-82 actually delivers lower radiation than a standard SPECT MPI study, because Rb-82 has an extremely short half-life of about 75 seconds. This is one reason ASNC guidelines now favor PET for repeat or serial imaging.
Side effects from either scan are uncommon. A few patients experience a brief warm sensation when iodinated CT contrast is injected. Allergic reactions to CT contrast occur but are rare. PET tracers are administered in micro-doses and are not associated with allergic reactions or kidney effects. The most common patient complaint about PET is the wait between injection and scan, during which patients are asked to rest quietly without using muscles.
How to Prepare for a PET or CT Scan
For a CT scan: if you are receiving IV contrast, you may be asked not to eat for 4 hours beforehand. Tell the imaging team if you have a history of contrast allergy, kidney disease, diabetes (especially if you take metformin), or are pregnant. Wear comfortable, metal-free clothing.
For a PET scan: most PET protocols require fasting for 4 to 6 hours before injection so background glucose levels are low and the tracer accumulates correctly. Avoid strenuous exercise for 24 hours before the scan, since muscle uptake interferes with image interpretation. Diabetics receive specific blood-sugar instructions; very high glucose levels can require rescheduling. For cardiac PET stress imaging, you may be asked to avoid caffeine for 12 to 24 hours. Plan for a 2- to 3-hour appointment.
Always follow the specific instructions your imaging center provides — protocols vary slightly by tracer, scanner, and clinical indication.

Frequently Asked Questions
Is a PET scan more accurate than a CT scan?
It depends on what you are looking for. For structural questions (bleeding, fractures, lung nodules, kidney stones), CT is the more accurate test. For functional questions (active cancer, viable heart muscle, dementia type), PET is meaningfully more accurate. Many patients receive both — fused into a single PET/CT study — to combine the strengths.
What can a PET scan show that a CT scan cannot?
PET can show whether a small lesion is metabolically active (likely cancer or infection) or metabolically silent (likely scar). It can show whether heart muscle is salvageable before a revascularization decision, distinguish Alzheimer's from frontotemporal dementia, and detect cancer recurrence inside post-treatment scar tissue — all situations where CT alone cannot give the answer.
Will a PET scan show all cancer?
No. PET is highly sensitive for most solid tumors but has known blind spots. Slow-growing tumors that consume little glucose (such as some prostate cancers, low-grade lymphomas, and certain neuroendocrine tumors) may not show up clearly on FDG PET. Specialized tracers — such as PSMA for prostate or Ga-68 DOTATATE for neuroendocrine — are used in those cases.
Why would my doctor order a PET scan instead of a CT scan?
Usually because they need to know how active or aggressive a known finding is, whether disease has spread to other parts of the body, whether treatment is working, or whether a finding is recurrent disease versus scar tissue. PET answers questions that CT cannot.
How long does a PET scan vs. a CT scan take?
A CT scan typically takes 5 to 30 minutes from start to finish. A PET scan takes 2 to 3 hours total — primarily because of the 45- to 60-minute tracer uptake wait between injection and imaging. The actual PET scan portion is 20 to 40 minutes.
Can you have a PET scan and a CT scan at the same time?
Yes — and it is the standard. A combined PET/CT scan acquires both image sets in a single appointment without the patient moving between scanners. The fused images are more accurate than either modality alone for cancer staging and certain cardiac and neurological indications.
Are PET and CT scans safe during pregnancy?
Both scans expose the fetus to ionizing radiation and are generally avoided in pregnancy unless the diagnostic information cannot be obtained any other way. Women of childbearing age should tell the imaging team if there is any chance they are pregnant. Ultrasound and MRI are usually preferred when imaging is needed during pregnancy.
Do PET and CT scans use the same contrast?
No. CT uses iodinated IV contrast (and sometimes oral barium or water-based contrast). PET uses an injected radiotracer — typically FDG for oncology or Rb-82 for cardiac perfusion — which works on a completely different principle. A combined PET/CT scan may use both: the radiotracer for the PET portion, and IV iodinated contrast if a diagnostic CT is also ordered.
Bring Mobile Cardiac PET to Your Practice
If you are a cardiologist or practice administrator deciding between sending patients out for cardiac imaging or bringing PET in-house, the math has changed in 2026. Mobile cardiac PET/CT lets your practice offer the most accurate non-invasive test for coronary artery disease — without the capital cost, build-out, or staffing burden of a fixed lab. Patients stay in your care across the imaging episode, and your practice captures the full reimbursement of the study.
Get in touch with VIP Imaging to learn how mobile cardiac PET/CT could work at your office — including a payer-specific reimbursement projection and a launch timeline.
Sources
- American Cancer Society. Understanding Radiation Risk from Imaging Tests.
- RadiologyInfo.org (RSNA & ACR). Radiation Dose from X-Ray and CT Exams.
- International Atomic Energy Agency. Radiation Protection of Patients During PET/CT Scanning.
- American Heart Association — Circulation: Cardiovascular Imaging. Diagnostic Accuracy of Cardiac PET vs. SPECT for Coronary Artery Disease.
- Society of Nuclear Medicine and Molecular Imaging / ASNC / SCCT. Joint Guideline for Cardiac SPECT/CT and PET/CT 1.0.
- National Center for Biotechnology Information (NCBI / StatPearls). PET Scanning.
- American Journal of Roentgenology. The Cost of Positron Emission Tomography in US Hospitals.
- GoodRx Health. How Much Is a PET Scan? Costs With or Without Insurance.