Cardiologist salary in 2026 is $630,000 at the median, with the full range spanning roughly $354,000 to more than $4.5 million depending on subspecialty, geography, and practice setting. Interventional cardiologists earn close to $690,000, electrophysiologists land between $650,000 and $750,000, and noninvasive cardiologists average about $470,000. The biggest swing factor — bigger than state, bigger than years of experience — is whether the cardiologist owns the revenue from the imaging and procedures they order. This guide breaks down current cardiologist income data from official sources, then shows you exactly how forward-thinking cardiology practices are using in-office cardiac PET/CT to add $1,000,000+ in annual practice revenue without taking on more call.
If you only have 60 seconds, here are the numbers:
- 2026 median cardiologist salary: ~$630,000
- 2026 average cardiologist salary: $575,000–$730,000 (varies by data source)
- Range: $354,000 (25th percentile) to $4,500,000+ (top earners)
- Top-paying specialty: Interventional cardiology and electrophysiology
- Top-paying setting: Private practice with imaging/procedural ownership
- Biggest income lever for 2026: Capturing in-office cardiac PET/CT reimbursement, which pays 4.4× more per patient than SPECT ($2,769.61 vs. $653.02 at 80% Medicare allowed) — enough to add $1M+ in annual practice revenue at typical volumes
How Much Does a Cardiologist Make in 2026?
The honest answer: it depends which dataset you trust. Cardiologist compensation surveys disagree because they sample different populations — recruiters see new offers, the BLS measures wage employees, and physician-reported databases capture late-career partners with full equity upside.
Here is what the major sources are reporting for 2026:
- SalaryDr (physician-reported) — Median / Average: $630,000 median · Notes: Updated 2026; includes private-practice equity
- ZipRecruiter — Median / Average: ~$357,000 average posted · Notes: Skewed by W-2 job postings
- U.S. Bureau of Labor Statistics — Median / Average: $421,300 mean (2023 data) · Notes: Federal wage data, lags by 2–3 years
- Marit Health — Median / Average: ~$575,000 average · Notes: 2026 physician-reported
- AMN Healthcare — Median / Average: $500K–$800K typical hospital range · Notes: Recruiter market data
Triangulating across these, $575,000 to $700,000 is the realistic 2026 cardiologist income band for a working full-time attending. The lower averages from job-board sources reflect base-salary postings only — they almost always exclude RVU bonuses, ancillary revenue, partnership distributions, and call pay, which together can add 30–50% to the headline number.
Cardiologist Salary by Specialty
Subspecialty is the single largest predictor of cardiologist pay. Procedural specialists out-earn noninvasive colleagues by $150,000–$250,000 per year because their work generates higher-RVU billings and ancillary imaging revenue.
- Interventional cardiology — 2026 Median Salary: $690,000 · Why: High-RVU cath lab procedures, call pay
- Electrophysiology (EP) — 2026 Median Salary: $650,000–$750,000 · Why: Ablations and device implants are top-paying CV procedures
- Structural heart / TAVR — 2026 Median Salary: $700,000+ · Why: Newer subspecialty; demand far exceeds supply
- Advanced heart failure / transplant — 2026 Median Salary: $500,000–$600,000 · Why: Concentrated in academic centers
- Noninvasive / general cardiology — 2026 Median Salary: $470,000 · Why: Office-based, depends on imaging revenue
- Cardiac imaging (echo, PET, CT, MR) — 2026 Median Salary: $500,000–$650,000 · Why: Imaging volume drives the upside
- Preventive / lipid — 2026 Median Salary: $350,000–$450,000 · Why: Lower procedural mix
Notice the imaging line. Cardiac imaging is the lever that lets a noninvasive or general cardiologist push compensation toward the high $600s without doing cath, EP, or transplant work — and it is the lever this article is going to spend the most time on, because cardiac PET reimbursement in 2026 is the single biggest underutilized income opportunity in cardiology today.
Cardiologist Salary by State
Geography matters, but less than people assume. After cost-of-living adjustments, the top-paying states are not always the highest-cost-of-living states:
- New York — Median Cardiologist Salary: $623,000 · Notes: High base, high COL
- California — Median Cardiologist Salary: $630,000 · Notes: High base, no state-tax advantage
- Texas — Median Cardiologist Salary: $580,000–$800,000 · Notes: No state income tax
- Florida — Median Cardiologist Salary: $480,000–$700,000 · Notes: No state income tax
- Nevada — Median Cardiologist Salary: Top 3 nationally · Notes: +64% vs. lowest-paying state
- Washington — Median Cardiologist Salary: $600,000+ · Notes: No state income tax
- Massachusetts — Median Cardiologist Salary: $590,000 · Notes: Concentrated in Boston academic centers
Per ZipRecruiter's state-by-state breakdown, the spread between the highest- and lowest-paying state is roughly $230,000. But a cardiologist in Texas earning $650,000 with no state income tax often takes home more than a New York cardiologist at $710,000 once you adjust for taxes and cost of living.
Cardiologist Salary by Experience Level
Cardiologist income compounds steeply in the first decade after fellowship and then plateaus once partnership equity matures.
- Cardiology fellow (training): $60,000–$75,000
- Year 1–3 attending: $400,000–$550,000 (many contracts include a base + RVU model with a 12–24 month guarantee)
- Year 4–7 attending: $550,000–$750,000 (productivity ramps, partnership track begins)
- Year 8–15 (full partner / senior employed): $700,000–$1.2M (ancillary distributions, ownership equity)
- Year 15+ (top decile): $1.5M–$4.5M+ (senior cath/EP partners, owners of imaging and ASC equity)
Median cardiologist income grew roughly 35% from 2014 to 2024 (per the American College of Cardiology compensation surveys). The fastest-growing segment was early-career cardiologists in private practices that own ancillary revenue — exactly the practices most aggressively adopting in-office cardiac PET.
Hospital-Employed vs. Private Practice Cardiologist Income
The split between hospital-employed and private-practice cardiologist income tells you everything about how to maximize earnings.
Hospital-employed cardiologists
- Higher base salary (often $700,000+)
- Predictable RVU model
- Benefits, malpractice, CME paid
- No upside on imaging, lab, or facility revenue
Private-practice cardiologists
- Lower base salary in early years
- Full upside on ancillary revenue: in-office echo, stress, nuclear, PET, CT, vascular, and ASC
- Partnership equity that can double effective compensation
- Invasive cardiologists in mature private practices regularly clear $825,000+ (AMN Healthcare 2026 data)
This is where the income strategy gets interesting. The single most leveraged decision a private-practice cardiologist makes is which ancillary services they bring in-house vs. refer out. Every cardiac PET scan referred to a hospital outpatient department is roughly $2,770 of professional + technical reimbursement that your practice will never see.
How Cardiologists Are Increasing Income in 2026: The Mobile Cardiac PET Opportunity
Here is the part most cardiologist salary articles miss entirely.
In 2026, cardiac PET/CT myocardial perfusion imaging is the highest-margin nuclear imaging modality available to cardiology practices, and it is dramatically underutilized. The American Society of Nuclear Cardiology's January 2026 updated clinical indications now name cardiac PET as the guideline-preferred test for evaluating coronary artery disease — a major expansion from prior guidelines that reserved PET for select scenarios. Major insurers reimburse PET myocardial perfusion imaging, and practices that offer PET/CT are now aligned with the latest clinical standards.
The clinical case is unambiguous. PET/CT delivers 88–91% diagnostic accuracy versus 70% for SPECT, in 45 minutes versus 3–4 hours, with lower radiation, sharper images for high-BMI patients, calcium scoring, multi-vessel and balanced-ischemia detection, and absolute myocardial blood flow quantification — none of which SPECT can match.
Combined with stable 2026 reimbursement under the CMS Hospital Outpatient Prospective Payment System (OPPS) Final Rule and the 2026 Physician Fee Schedule, the financial case is now overwhelming.
Cardiac PET vs. SPECT: The Real Revenue Math
Here is the line-item breakdown at 80% Medicare allowed reimbursement, the way it actually shows up on your remits:
- Primary perfusion code — SPECT: 78452 — $478.26 · PET/CT: 78452 — $2,170.96
- Radiopharmaceutical (rest + stress) — SPECT: A9500 — $243.16 · PET/CT: A9555 — $1,041.50
- Stress test — SPECT: 93015 — $82.77 · PET/CT: 93015 — $82.77
- Lexiscan — SPECT: J2785 — $12.08 · PET/CT: J2785 — $12.08
- Absolute quantification (MBF) — PET/CT: 78434 — $154.70
- Patient total (100% allowed) — SPECT: $816.27 · PET/CT: $3,462.01
- 80% Medicare allowed — SPECT: $653.02 · PET/CT: $2,769.61
- Exam time — SPECT: 2–4 hours · PET/CT: 45 minutes
- Diagnostic accuracy — SPECT: ~70% · PET/CT: 88–91%
That is 4.4× more revenue per scan for the same clinical question, with shorter exam times, lower patient radiation, and dramatically higher diagnostic confidence. For the deep dive on every CPT code (78429, 78430, 78431, 78432, 78433, 78434) and Rubidium-82 generator pricing (HCPCS A9555), see VIP Imaging's Cardiac PET Reimbursement 2026 Guide.
What This Looks Like in Real Cardiologist Income
The deck math is straightforward. At a typical cadence of 15 patients per PET day and a Medicare-blended $2,855 average reimbursement per scan, one PET day generates $42,825 in gross practice revenue. Stack PET days across the year and the picture compounds:
- Worst case — Net Profit / Patient: $1,200 · Patients / Day: 15 · Days / Year: 48 · Annual Net Profit: $864,000
- Average case — Net Profit / Patient: $1,516 · Patients / Day: 15 · Days / Year: 48 · Annual Net Profit: $1,091,520
That is $864K to $1.09M in net annual practice profit flowing into physician compensation, from a service line that runs one day per week and that you currently refer out. Cardiology practices on the VIP program typically see imaging volume increase 25–50% in the first 12 months as PET indications broaden the addressable patient population.
This is not theoretical. It is what cardiologists who have already added in-office cardiac PET are reporting:
"We doubled our nuclear cardiology revenue in the first six months. The VIP team handled everything — scheduling, billing, and compliance. We just focused on our patients." — Dr. Rajesh Chawla, Cardiologist (2× revenue growth)
"Our practice saw a 75% increase in revenue within the first year. The concierge model is unlike anything else in the market — they truly operate as an extension of our team." — Dr. Brian Chesnie, Cardiologist (+75% revenue increase)
"The most accurate cardiac imaging I've ever had access to. My patients are getting better diagnoses, and my referrals have increased significantly since we started the program." — Dr. Fernando Mendoza, Cardiologist (#1 in imaging accuracy)
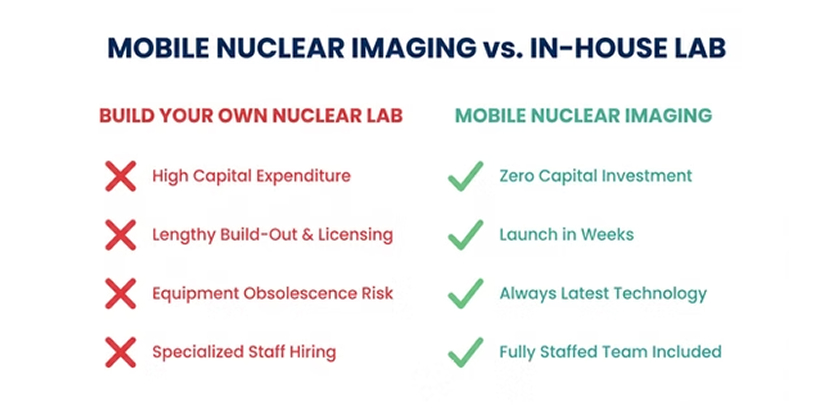
The Catch: Owning the Equipment Is a $2M+ Mistake
The reason most practices do not capture this revenue is straightforward. Building your own in-house PET/CT program means a $1.5–$2.5M camera plus a shielded suite plus a full-time nuclear medicine tech plus weekly Rubidium-82 generator orders — the kind of overhead that only pencils out if you are running PET five days a week.
Here is what the real DIY math looks like, line by line, against a turnkey VIP partnership:
- PET/CT camera (7% interest, 5-yr payoff) — DIY (Build It Yourself): $27,724 · VIP Partnership: Included — no capital
- Camera maintenance / service contract — DIY (Build It Yourself): $11,667 · VIP Partnership: Included
- Nuclear-med staff salaries + benefits — DIY (Build It Yourself): $6,807 · VIP Partnership: Included
- Rubidium-82 generator — DIY (Build It Yourself): $50,000 · VIP Partnership: Included
- Reading software (2-yr license) — DIY (Build It Yourself): $833 · VIP Partnership: Included
- Supplies ($30 × 60 patients/mo) — DIY (Build It Yourself): $1,800 · VIP Partnership: Included
- Loss of two clinical rooms (opportunity cost) — DIY (Build It Yourself): $34,667 · VIP Partnership: $0 — mobile unit
- Total cost per patient — DIY (Build It Yourself): $2,225 · VIP Partnership: $1,600
- Total cost per year — DIY (Build It Yourself): $1,601,976 · VIP Partnership: $1,152,000
- Savings with VIP — VIP Partnership: $625/patient · $37,498/mo · $449,976/year
For a practice doing 1–3 PET days per week, owning the equipment leaves roughly $450,000 per year on the table versus partnering. This is why mobile cardiac PET/CT has become the dominant adoption model in 2026.
How VIP Imaging Helps Cardiologists Increase Income
VIP Imaging — headquartered in Anaheim, California — is the largest mobile nuclear cardiac imaging company in the western United States, serving cardiology practices across California, Arizona, and Texas. We call ourselves the pacemaker of cardiac imaging: the best test possible, delivered to your practice.
The model is fully turnkey. On the day(s) you schedule, VIP brings everything you need to run a hospital-grade cardiac PET program inside your existing office:
- PET imaging equipment — the United uMI 550 digital PET/CT scanner (2020+ generation, 2.9 mm spatial resolution, lifetime software upgrades, contractual uptime guarantee). Fits inside standard physician offices — no shielded suite construction, no real-estate commitment.
- Certified imaging technologists — VIP-trained and credentialed staff, on-site for the day.
- Rubidium-82 (RB 82) generator and all consumables — including Lexiscan, IV supplies, and isotopes. We bring it in, we take it away.
- Scheduling and patient coordination — VIP manages your PET-day calendar to maximize throughput and minimize gaps.
- Billing and pre-authorization support — our team handles prior auths so your staff is not buried in payer paperwork, and ensures correct CPT coding to capture full reimbursement on every scan.
- Dedicated concierge support, start to finish — a real person guiding setup, billing, reimbursement, and on-site operations.
- Reading on the gold-standard platform — acccess to 4DM and Cedars-Sinai cloud-based software, 24-hour read turnaround, accessible from any internet-connected device.
The result: your practice captures the full $2,769.61 per-scan reimbursement that a hospital outpatient department captures, without the capital outlay, without the staffing burden, and without your team having to learn nuclear medicine operations.
For the operational walkthrough, see VIP's article on mobile nuclear imaging delivered directly to your practice. For the implementation roadmap with timelines, scheduling strategies, and what to expect in the first 90 days, see How to Bring Cardiac PET/CT to Your Practice: 2026 Guide.
Which Patients Qualify for PET? (Hint: Most of Them)
A common misconception is that PET should be reserved for complex or failed-SPECT cases. The 2026 ASNC guidelines reframe this: PET should be the first test, not the last test.
Patients who qualify include:
- Coronary artery disease (CAD) / ischemia evaluation
- Undiagnosed chest pain
- Obese patients (BMI > 30) — where SPECT image quality breaks down
- Abnormal EKG or abnormal stress test
- Suspected microvascular disease
- Cardiomyopathy evaluation
- Prior stent or bypass surgery
- Prior false-positive or false-negative SPECT
- Pre-op cardiac risk assessment
- Patients unable to exercise (pharmacologic stress)
- High-risk symptomatic patients
- Suspected multi-vessel disease
In other words: the same indication list as SPECT, with superior accuracy. Start with confidence, not uncertainty.
What a Mobile Cardiac PET Engagement Adds to Cardiologist Income
A practice that schedules one PET day per week with VIP, scanning 12–15 patients per day at the average-case Medicare-blended rate, generates roughly $1,000,000+ in net annual practice profit that did not exist before — because that revenue used to walk out the door to a hospital outpatient department. For a four-cardiologist group, that is roughly $250,000+ per cardiologist per year added to compensation, in exchange for one scheduled day per week of imaging that mostly runs itself. For a solo or two-physician practice, the per-cardiologist impact is meaningfully larger.
Add to that the 25–50% imaging-volume lift practices typically see in year one as PET indications broaden the patient pool, and the income story compounds quickly.
This is why "cardiologist salary" of the future increasingly comes down to a single decision: do you keep referring nuclear studies out, or do you bring the camera in?
Cardiologist Salary FAQs
What is the average cardiologist salary in the U.S. in 2026?
The average cardiologist salary in the United States in 2026 is approximately $575,000–$700,000, with a median of $630,000 according to physician-reported data from SalaryDr. Government wage data from the Bureau of Labor Statistics reports a lower mean of $421,300 because it lags by 2–3 years and excludes private-practice partner distributions.
How much does an interventional cardiologist make?
Interventional cardiologists earn a median of approximately $690,000 in 2026, with experienced interventionalists in private practice regularly exceeding $825,000. Compensation is driven by high-RVU cath lab procedures, call coverage, and ancillary revenue from cardiac imaging.
What is the highest-paid cardiology subspecialty?
Structural heart (TAVR, MitraClip), electrophysiology, and interventional cardiology are the highest-paid subspecialties, all clustering between $650,000 and $800,000+ at the median. Top-decile partners in mature private practices with imaging and ASC ownership can exceed $2,000,000.
Do cardiologists make more in private practice or hospitals?
Hospital-employed cardiologists usually have higher base salaries, but private-practice cardiologists with partnership equity and ancillary revenue ownership consistently out-earn hospital peers in the long run — often by $200,000–$500,000 annually once cardiac imaging, lab, and ASC distributions are included.
How can cardiologists increase their income?
The highest-leverage income strategy for cardiologists in 2026 is bringing high-reimbursement imaging in-house — particularly cardiac PET/CT, which reimburses 4.4× more per patient than SPECT ($2,769.61 vs. $653.02 at 80% Medicare allowed). At 15 patients per PET day, one day per week with a mobile partner like VIP Imaging generates roughly $1M+ in annual practice profit without the $2M+ capital outlay of buying a fixed PET/CT system.
What is cardiac PET reimbursement in 2026?
Cardiac PET myocardial perfusion imaging reimburses approximately $2,769.61 per patient at 80% Medicare allowed under the 2026 CMS fee schedules ($3,462.01 at 100% allowed), compared to about $653.02 for a SPECT study — a 4.4× revenue advantage per patient. Primary CPT code 78431 was held stable in the 2026 OPPS Final Rule, and the high-cost radiopharmaceutical pass-through policy continues. See VIP Imaging's Cardiac PET Reimbursement 2026 Guide for the full CPT-by-CPT breakdown.
Is cardiology worth the training for the salary?
For most cardiologists, yes. Median lifetime earnings for a cardiologist typically range from $18 million to $25 million over a 30-year career, comfortably justifying 10–12 years of post-college training and the average $250,000–$400,000 in medical school debt. The career also has favorable demand fundamentals: BLS projects 4.1% job growth through 2034, and 46% of U.S. counties currently lack a single cardiologist.
The Bottom Line on Cardiologist Salary in 2026
Cardiologist income in 2026 is not just a function of where you trained or what subspecialty you chose — it is increasingly a function of which revenue streams you choose to capture inside your own practice. The cardiologists pulling away from the median are the ones who realize that the 4.4× revenue gap between in-office cardiac PET and outsourced SPECT is, in dollar terms, larger than the gap between general and interventional cardiology compensation.
If you are a cardiologist looking to add $1,000,000+ in annual practice revenue without taking on more call, more weekends, or more capital risk, mobile cardiac PET/CT is the most direct lever available in 2026.
Talk to VIP Imaging about scheduling cardiac PET/CT days at your practice. Phase 1 is risk-free: launch SPECT on your schedule, experience PET firsthand with a Demo Day, and get a free custom reimbursement analysis showing the real numbers for your practice (a $2,500 value). No commitment required — evaluate entirely on your terms. Or read the full implementation guide to see what bringing PET in-house looks like, end to end.
Sources
- U.S. Bureau of Labor Statistics — Cardiologists (OES 29-1212)
- SalaryDr — Cardiology Compensation 2026
- ZipRecruiter — Cardiologist Salary
- Marit Health — Cardiologist Salary 2026
- AMN Healthcare — Interventional vs. General Cardiologist Salary 2026
- CMS — 2026 Hospital OPPS Final Rule
- CMS — Physician Fee Schedule Search
- American College of Cardiology — 2026 OPPS Highlights
- American Society of Nuclear Cardiology — Reimbursement & Coverage